The headlines on hospital discharge make for depressing reading. Prolonged stays in hospital are associated with worse health outcomes and increased care. Ten days of bed-rest in hospital, is the equivalent of 10 years of muscle ageing for people 80+. The numbers of people waiting in hospital for support on discharge have significantly increased over the years with around £820 million a year delayed hospital stays (National Audit Office).
Levels of demand on health and social care services are rising while Adult Social Care departments have had their budgets significantly cut. There is sector wide recognition that more funding is required, and this sense of urgency has permeated government ranks. The system needs more investment but this is not a single fix. Much closer and integrated working between all organisations involved in hospital discharge will help to reduce delays and there have been some excellent initiatives nationally. Many programme managers and project managers have been recruited through Sustainability and Transformation Partnerships and Better Care Fund Plans to identify with senior managers local solutions to the complex issue of hospital discharge.
However, my experience working for many years in this area has been that information on new initiatives and knowledge around best practice in hospital discharge is not always being cascaded down to those directly responsible day to day for supporting hospital discharge, in part because of challenges to release staff from frontline practice. Often those working directly with people have no idea about the vision and plans for better integrated solutions to hospital discharge let alone are invited to be part of the conversations about best practice in hospital discharge.
My experience is that many practitioners are not made aware of some of the pilots and new services set up to support hospital discharge. Indeed, working with Adult Social Care Departments and NHS acute and community organisations over the past few years on hospital discharge it’s clear that many practitioners and their managers are still unaware, for example, of NICE guidelines and recommendations around hospital discharge, reablement and intermediate care and best practice evidenced nationally by organisations such as NHS Improvement, the Kings Fund and the Social Care Institute for Excellence.
A National Audit Office report published in May 2016 stated that “Health and social care providers have made limited progress in adopting recommended good practice”.
Basic good practice recommendations such as starting discharge planning early, identifying blocks to discharge early in the admission and making sure the person is informed and in control are still not consistently adhered to. Often those facilitating discharge are not supported to work together with their community colleagues to ascertain how people were being supported before admission or to ensure they are properly supported on discharge. Far too many assessments and decisions for long term care and whether people will benefit from reablement and rehab, for example, are still being made in an unfamiliar hospital environment despite the push for discharge to assess models.
A couple of weeks ago I was charged with delivering training on recording delayed transfers of care to front line local authority workers. They were clearly very committed and passionate about providing good hospital discharge support. What they wanted was to know about the technical aspects of the legislation, so they could “challenge” their NHS colleagues on numbers of DToCs. What they needed was to understand the impact on health and wellbeing of those people delayed in hospital while they “challenged”. They needed to be empowered to develop closer working relationships with their NHS colleagues both operationally and in understanding each other roles and remits and increasing their knowledge and skills around best practice in integrated working and hospital discharge.
Without staff being supported to develop in line with evidence-based practice, ways of working will remain static with staff from different organisations continuing to practice inconsistently and separately despite the best efforts of the senior managers and project managers to “integrate” services.
Change has to come from the bottom up as well as at a senior operational or strategic level, with health and social care front line workers being given the skills, knowledge and forums to learn together about evidence-based practice in hospital discharge and intermediate care services. Nothing will change otherwise and no matter how much money is invested and how many great initiatives are piloted, and many people will continue to experience poor hospital discharges.
Over the last few years, we have had the opportunity to work in a more integrated way with health services in our course development. Supported by health and social care practitioners we have been considering how health and social care interact; the cause and effect, the impact and outcomes on a practice level within specific domains. This interlocking enables us to develop new insights and tools. Within this we have been considering:
What are the individual and collective benefits to services of receiving more support for exercise for people living in with dementia?
What are the potential barriers to providing exercise in care homes and/or community settings?
What priority is given to this and what training is available to facilitate this?
Health and Wellbeing is identified in the Dementia Care Skills Education and Training Framework (section 6), as a key area for education and development for staff working with people with dementia both at tier one and tier two. Section 6 includes health as well as psychosocial activities as expected, and exercise is explicitly mentioned in the first outcome. We have interpreted the outcomes to a more meaningful and measurable course outcome, with exercise linking to many other aspects identified within this section, including but not limited to falls and pain management. Alongside my health colleagues we have debated and developed the merits and outcomes of this course which is set to be a very practical and holistic look at front line integrated interventions.
The Context
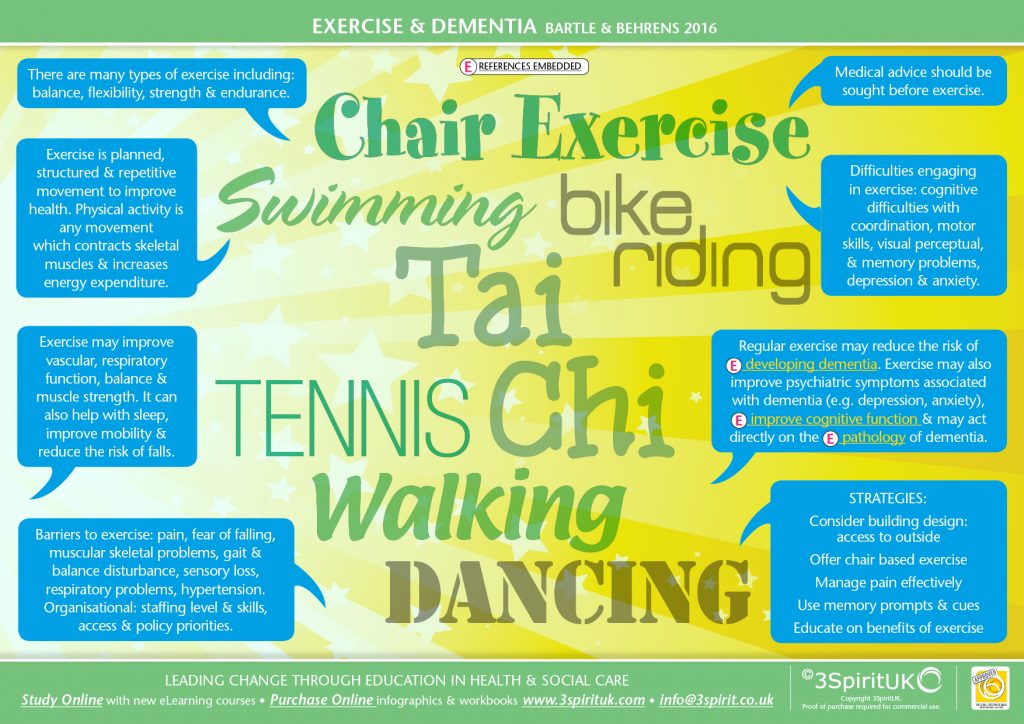
Over the last few years there has been some exciting research emerging about the impact of exercise on dementia. Alongside which we have started to see exercise offered in front line services as part of prevention strategies. In addition, policy and legislation changes such as the Care Act 2014 have outlined their vision for prevention, of which exercise must feature. Organisations like Age UK have offered chair based exercise, and exercise has been targeted by some authorities as an intervention to reduce the risk of falls and other health outcomes.
The emergence of more collaborative working between health and social care has stimulated the growth of such initiatives; pooling funding to improve health outcomes with prevention. However, what is emerging from the research is that exercise potentially has much wider benefits than reducing the risk of falls, particularly in terms of its application to dementia. Mental health services and local primary care services have offered exercise on prescription for many years as a valid form of treatment for depression, so exercise may potentially offer a valid treatment for some of the neuropsychiatric disorders which often are associated to dementia for example; depression, apathy, hyperactivity and agitation. Exercise may also enable improvements in cognition, and some research seems to suggest that exercise may act directly on the pathology of dementia. What is very clear however is that exercise has far reaching impacts both for physical and mental wellbeing.
Some Definitions
Exercise is planned, structured and repetitive movement which aims to improve or maintain physical health. Physical activity is any movement which contracts skeletal muscles and increases energy expenditure. The main types of exercise are aerobic, strength, flexibility and balance. Aerobic exercise increases breathing and heart rate. Strength exercises make your muscles stronger. Balance exercises can help prevent falls and flexibility exercises help you to remain limber and improve the range of movement.
The Barriers
However, accessing and maintaining activity where comorbidity is present can be a challenge. If a person is older when they develop dementia they may also experience barriers to accessing and maintaining exercise. For example, pain, fear of falling, arthritis, sensory loss, or respiratory problems. A person may also have restricted movement and some rigidity and quite possibly not be mobile. Good assessment, including pain assessment should be completed to develop a plan that is appropriate to that individual alongside advice from the GP. However not all people developing dementia are older, so this could exercise may be an excellent targeted intervention for younger people with dementia? A study in the Netherlands is currently researching the impacts of exercise in early on set dementia (EXERCISE-ON study) the authors (Hooghiemstra et al 2012) suggest that certain dementia characteristics such as apathy may lead to sedentary and socially impoverished lifestyles, and by targeting these interventions in a timely fashion they can have far reaching impacts.
Together with co-morbidity barriers, we need to consider the challenges dementia brings in potentially engaging in exercise. For example, difficulties with coordination, motor skills, visual perceptual challenge and memory difficulties. These difficulties will require us to have a considered approach to the support systems needed to overcome these challenges.
There is such a wide variety of exercise available to us therefore it is about identifying strengths, and identifying suitable exercises that engage these strengths. This might include walking, dancing and/ or using music. Music can powerfully evoke memories, impact on motivation as well as provide rhythm and structure to support difficulties with memory. It is therefore an excellent method of exercise.
The Benefits
Exercise may improve thinking skills. A Chinese study (Lam et al 2012) found that mind-body exercises such as Thai Chi could improve cognition as well as have additional impacts such as improving balance and strength. Exercise is targeted as a potential primary prevention strategy to delay / reduce onset of dementia once someone has been diagnosed with mild cognitive impairment. The wider impacts of exercise on health outcomes are well documented, despite this many services fail to see the importance of it, and more specifically their role in supporting and enabling exercise.
Some studies have been completed to look at how effective exercise is in care homes at reducing the incidence of depression. Depression impacts on quality of life and pharmacologic treatments are not without their side effects. Some studies have found no evidence that moderate exercise in a care home had an impact on depression (Conradsson et al 2010). In contrast Edris et al (2009) had more success in providing a three week exercise plan, as found that it reduced levels of agitation. Agitation and depression are not directly comparable, and clearly variables will differ within this context. However, reducing incidences of agitation could have a direct impact on staff costs associated to working with challenge. Researching the impact of exercise on depression within a care home is a complex task, as the social environment, beyond the time of the exercise will potentially impact. Separating these variables in research is bound to be a challenge.
Conclusion
Despite the barriers, both in research and in delivery opportunities for people living in care homes to exercise must continue to be a priority. Factors to be considered include: building design, access to outdoors, effective pain assessment and management, and education on the benefits of exercise. There may be a wider impact on these enablers, including improved mood, better sleep and potentially improved nutritional intake.
Are you interested in knowing more about this course then click here
If you would like to hear about other courses click here
Bibliography
Ahlskog, E.J., Geda, Y.E., Graff-Radford, N.R. and Petersen, R.C. (2011) ‘Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging’, 86(9).
Aman, Edris et al.(2009) ‘Supervised Exercise to Reduce Agitation in Severely Cognitively Impaired Persons’, Journal of the American Medical Directors Association , Volume 10 , Issue 4 , 271 – 276
Baker, L.D., Frank, L.L., Foster-Schubert, K., Green, P.S., Wilkinson, C.W., McTiernan, A., Plymate, S.R., Fishel, M.A., Watson, S.G., Cholerton, B.A., Duncan, G.E., Mehta, P.D. and Craft, S. (2010) ‘Effects of aerobic exercise on mild cognitive ImpairmentA controlled trial’, Archives of Neurology, 67(1), pp. 71–79. doi:
Conradsson, M., Littbrand, H., Lindelöf, N., Gustafson, Y. and Rosendahl, E. (2010) ‘Effects of a high-intensity functional exercise programme on depressive symptoms and psychological well-being among older people living in residential care facilities: A cluster-randomized controlled trial’, Aging & Mental Health, 14(5), pp. 565–576
Duzel, E., van Praag, H. and Sendtner, M. (2016) ‘Can physical exercise in old age improve memory and hippocampal function?’, 139(3).
Hoffmann K, Frederiksen K, S, Sobol N, A, Beyer N, Vogel A, Simonsen A, H, Johannsen P, Lolk A, Terkelsen O, Cotman C, W, Hasselbalch S, G, Waldemar G, Preserving Cognition, Quality of Life, Physical Health and Functional Ability in Alzheimer’s Disease: The Effect of Physical Exercise (ADEX Trial): Rationale and Design. Neuroepidemiology 2013;41:198-207
Hooghiemstra, A.M., Eggermont, L.H., Scheltens, P., van der Flier, W.M., Bakker, J., de Greef, M.H., Koppe, P.A. and Scherder, E.J. (2012) ‘Study protocol: EXERcise and Cognition in sedentary adults with early-oNset dementia (EXERCISE-ON)’, BMC Neurology, 12(1), p. 75.
Littbrand, Hã., Lundin-Olsson, L., Gustafson, Y. and Rosendahl, E. (2009) ‘The effect of a high-intensity functional exercise program on activities of daily living: A Randomized controlled trial in residential care facilities’, Journal of the American Geriatrics Society, 57(10), pp. 1741–1749
Lam, Linda C.W. et al (2012) ‘A 1-Year Randomized Controlled Trial Comparing Mind Body Exercise (Tai Chi) With Stretching and Toning Exercise on Cognitive Function in Older Chinese Adults at Risk of Cognitive Decline’ Journal of the American Medical Directors Association , Volume 13 , Issue 6 , 568.e15 – 568.e20
Lowery, D., Cerga-Pashoja, A., Iliffe, S., Thuné-Boyle, I., Griffin, M., Lee, J., Bailey, A., Bhattacharya, R. and Warner, J. (2013) ‘The effect of exercise on behavioural and psychological symptoms of dementia: The EVIDEM-E randomised controlled clinical trial’, International Journal of Geriatric Psychiatry, 29(8), pp. 819–827.
Schwenk, M., Dutzi, I., Englert, S., Micol, W., Najafi, B., Mohler, J. and Hauer, K. (2014) ‘An intensive exercise program improves motor performances in patients with dementia: Translational model of geriatric rehabilitation’, Journal of Alzheimer’s Disease, 39(3), pp. 487–498
Last week the Kings Fund and Nuffield Trust produced a report, ‘Home Truths’, demonstrating the impact of the local authority spending cuts over the last six years on social care. The report highlights the combined pressures on services, such as maintaining Fundamental Standards (CQC), working towards achieving the Living Wage, dealing with contract cuts, as well as coping with significant staffing shortages. Cumulatively these pressures have meant that many services have fallen short of demand and for some there have been serious failings. However, for the majority, the shortcomings are visible in delayed discharges from hospital, which has a negative fiscal impact.
The report highlights some of the strategies adopted by services to compensate for these cuts. For example, some providers are relying more heavily on privately funded clients to subside their local authority contracts. Some are actively identifying options for support in the wider communities and using volunteers to bolster their service.
The report warns that the social care sector will not cope against the continued planned cuts and additional sector pressures, and recommends three possible options to address the dismal outlook:
achieving more with less
a different offer
long term reform
Whilst the latter two can be debated over the longer term by politicians and senior social care figures alike, providers need to be getting on with the ‘what can we achieve for less’ more imminently. There is an urgent and critical need to think outside the box about how we can do things differently.
As part of the ongoing strategic review many services have been actively reviewing their resource input against their outputs and outcomes in an attempt to get more for less. Good business strategists understand that the skill lies in leveraging resources effectively to create a comfortable operating profit. This isn’t always about cutting back but rather doing things differently. Training is one example of a resource that can be manipulated for different outcomes. There has been a growing reluctance to spend on training, with more services opting instead to develop independent capabilities or deliver E learning in the hope that this widens the profit margin. However, in reality some of these ‘cutting corner’ decisions can impact on quality, leaving services ill prepared to ‘fire fight’ issues such as safeguarding incidences, health and safety concerns, complaints and/or poor service outcomes. Many of these matters often rear their ugly head at a time when services are logistically challenged, forcing the focus on resources toward just covering the job instead of on maintaining and improving outcomes.
On a more strategic level, within our local area some excellent joined up thinking has been going on. Integrated projects have developed, which have been supported by the pooling of NHS funding (Better Care Fund), aiming for smarter working through integrated practice. Our organisation has been involved in one of these projects, working with care homes to reduce hospital admissions. Hospitals are very disabling places for people living with dementia, and poor outcomes are typically observed; economic and individual. Clearly there is a lot of work to be done to upskill staff to ensure that there is a timelier reporting of health concerns through better quality observations, and ensuring that preventative measures are put in place to avoid unnecessary admissions.
One of the areas that has seen the largest cut in funding is community based services, such as support at home (homecare). Spending is down a whopping 30% despite policy objectives to support more people in the community. This is a significant cut in comparison to residential and nursing services which were only cut by 4 – 6%. Home care services now are delivering more hours for less money. So what solutions are there available for our home care services?
This key question has been the driving force behind the development of Home Spirit, a platform developed for home care providers. The platform equips services with the tools to literally think differently, be proactive and add value to their service.
The portal consists of a number of tools. The person centred planning tool has several potential domains which are selected by the client, and are based on their specific identified outcomes. It is easy to use and prints and uploads reports, making sharing easy. It avoids duplication, or having to write anything out so saves time. It can be completed on mobile while at the client’s home, and, with an easy to use navigation system, it has sensory appeal. The tool helps agencies to reduce operational costs in assessment and reporting. It can highlight risks easily, both those that are determined by the individual as well as the care agency. The report can be produced in a shorter version (similar to a one page profile) which informs busy workers in a simple snapshot HOW to provide the support. At £19 per month for as many reports as required, it is also excellent value.
The environment audit is intended to be a proactive tool. It may reduce hospital admission and risk of falls through environment assessment. It can be used by families and individuals to identify potential assistive technologies (a requirement of the NICE Home Care guidelines 2015), which include health monitoring options, safety and activity monitors, and leisure and communication technologies. These technologies now have a much wider scope and can promote human connection and tackle loneliness. Loneliness has been linked to poor health outcomes, leading to additional financial burdens on community and NHS services. Tackling loneliness through supported use of assisted technologies is only one of the many benefits that can be introduced by the tool. The environment audit tool also makes simple recommendations for environmental adaptation to improve independence. The environment tool will also make recommendations around how an environment can be adapted around a specific task for a person with dementia, and therefore informs and educates, offering a tailored support plan.
The ‘still my life’ post diagnostic tool is completely FREE to access and helps families to plan together to take proactive steps to manage the condition; this aims to reduce anxiety. One of the first questions asks the person to consider the difficulties they face and what actions they plan to put in place to mediate these challenges. The design of the tool aims to encourage people to rehearse their own strategies, helping them recall them with more proficiency, as well as have very clear goals on how to compensate for their difficulties. Another question prompts the person to consider aspects of life that they appreciate and value (positive psychology), this can have a direct therapeutic value. One of the questions guides individuals to complete appropriate legal planning. Local authority resources spent making ‘best interest’ decisions could be avoided by documenting decisions in a timelier manner. The planning tool provides accessible guidance on how these measures can be put into place. The tool also asks individuals to consider early interventions for nutrition and sleep. As 72% of people living with dementia are also living with another condition (co-morbidity), early strategies to support sleep and nutrition can have a positive effect, reducing risks of delirium and inappropriate admissions to hospital. The post diagnostic planning tool can be easily downloaded and completed on paper. This additional tool is potentially an asset to home care providers, as providing access to this resource as part of your service shows that you provide added value. Perhaps more importantly a tool like this provides hope, and motivates families and individuals to think proactively.
The circle of support tool helps to identify communities of support to build upon existing community networks and engender a sense of belonging and affiliation to the wider community.
The learning resources (infographics) available through the portal support staff, through bite-size learning, to observe better, develop better relationships, and improve reporting. The flexible resource reduces the need for staff to be removed for training at critical pressure times. Community services are now working with higher levels of need and the skills sets required are reflective of this. Appropriate investments need to be made in knowledge management. The resources available on this portal are specifically designed to work well in busy environments.
Therefore, while services are scratching their heads considering their next move to survive this hostile environment, we have been actively developing a solution. The benefits of the Home Spirit tool are potentially far reaching and offer a legitimate opportunity to services to do things differently and to achieve more for less.
According to the Department of Health (2013) there are an estimated 15 million people with long term conditions which cannot be cured including dementia, hearing loss, diabetes, sight loss, stroke. In many cases long term conditions are linked to the ageing process.
Age-related damage is the single biggest cause of hearing loss, and 44% of over-70 year olds have moderate to severe hearing loss (Joining up, action on hearing loss). People with hearing loss have problems recognising speech, especially in challenging environments. They need to concentrate more than people with normal hearing to pick up as much as possible from the acoustical world (Arlinger 2003).
Uncorrected hearing loss gives rise to a poorer quality of life, reduced social activity, and increased symptoms of depression.
There are almost 2 million people living with sight loss in the UK. Sight loss may be due to long term conditions. For example diabetes: over 1 in 20 people in the UK have diabetes and are at risk of sight loss (diabetic retinopathy). It is estimated 60% of people following a stroke have visual problems. Sight loss is linked to age with 1 in 5 people over the age of 75 living with sight loss (Access economics 2009).
Difficulties with vision are not always obvious. Signs of sight loss might include:
Person reports flashing lights or patterns in front of their eyes
Peering closely at faces and print
Needs brighter lighting
Moves more slowly: stumbling
Starts to touch objects and people to find way around
Sight loss impacts upon a person’s wellbeing including increasing the risk of social isolation and risk of injury through falling: visual impairment is associated with falls and hip fractures. NICE has emphasised the importance of visual assessment in prevention of falls (NICE CG 161 June 2013: Falls in older people: assessing risk and prevention).
Appropriate lighting may help to reduce the incidence of falls. By the age of 75 a person needs four more times the light that a person needs when they are 20. As the eye gets older it has more difficulty managing glare and changes to light levels, therefore avoiding sudden changes in light levels will help.
Addressing communication needs is essential to enable people to play a role in managing their long term conditions: for example diabetes. As older people may have co-morbidities and sensory loss, there are implications for services: Services may need to consider how to support a person’s sensory loss to ensure they may understand information about their condition and how they may manage their condition.
The greater the age of a person, the greater the risk of developing a dementia: 820,000 older people have a diagnosis of dementia in UK (Alzheimer’s Society) and therefore older people may have dementia, sight and hearing loss. Dementia, together with sensory loss, can make communication more difficult.
Some types of dementia can cause visual problems and sight loss may make the effect of dementia appear more pronounced.
A person living with dementia uses their sensory and cognitive skills to understand the world around them. If one aspect is damaged, for example cognitive skills, a person with dementia becomes more reliant on their sensory skills to transfer information to the brain to help them make sense of the world around them. The analysis of the information will be impaired if the person has damage to certain lobes of the brain: for example: if there is damage to the occipital lobe, the person may have difficulty recognising an object or with colour contrast. These difficulties are known as ‘visual perceptual problems’, and may present as illusions, misinterpretations or misidentifications.
A person that is older, and living with dementia, may need additional help to manage their sight loss and/or hearing loss. Problems with memory may mean that the person forgets to put their glasses on, or forgets where their glasses are. Memory aids visual or auditory (e.g. recorded message) may be helpful. A person living with dementia will uses clues in the physical environment to understand what they are doing, or what is happening next. Appropriately supporting sensory skills may help them to do this.
Helen Behrens (Trainer 3 Spirit UK)
Access Economics, (2009). Future Sight Loss UK 1: The economic impact of partial sight and blindness in the UK adult population. RNIB.
Department of Health (DH) (2013) Improving quality of life for people with long term conditionshttps://www.gov.uk/government/publications/2010-to-2015-government-policy-long-term-health-conditions accessed 7/01/2016
Arlinger S (2003) Negative consequences of uncorrected hearing loss––a review International Journal of Audiolog; 42:2 S17–2 S20
As health and social care trainers we straddle the medical and social model, and believe whole heartedly, holistic, and integrated practice is required to enable positive outcomes, and well-being within our communities. Within each realm of medical and social perspective, many factors which may be viewed in isolation maybe interdependently linked: manipulating one factor, may impact upon others. We need to take a balanced approach, informed by consent, and at times, pharmacological strategies are warranted, and at others times we should consider non-pharmacological approaches.
It is our responsibility, within training sessions, to encourage staff to reflect upon their clients and the complex nature of the conditions, to equip them with skills to observe, report and signpost. One subject raised within sessions is polypharmacy. Many of the services we train are commonly working with comorbidity, and complexities around fluctuating sates, often resulting in competing care and treatment strategies. To support discussions relating to polypharmacy, we developed some resources with the aim to get people to think and reflect more broadly about the topic.
Inappropriate polypharmacy is a very real and present threat, as many prescribing practitioners face tensions between treating common conditions and the risks associated with polypharmacy.
Many people with dementia, together with older population are affected by polypharmacy. Older people generally will have multiple health conditions which require medication. However, given the potential communication difficulties presented with dementia, particularly around problematic pain management, it is possible that there is a higher prevalence of polypharmacy in this group.
There is no clear definition for Polypharmacy: Sometimes numerical: for example greater than 6. Accepting a numerical definition of polypharmacy has the disadvantage: does not recognise that in some cases the combination use of certain medications is beneficial to the older person. Inappropriate polypharmacy is when the person takes more drugs than are clinically indicated.
Polypharmacy is a concern in this group because there are age-related physiological changes that alter the ways in which drugs are handled by the body. This may include:
• Reduced renal function
• Reduced liver function
• Reduced ratio of body fat to water
• Delayed stomach emptying
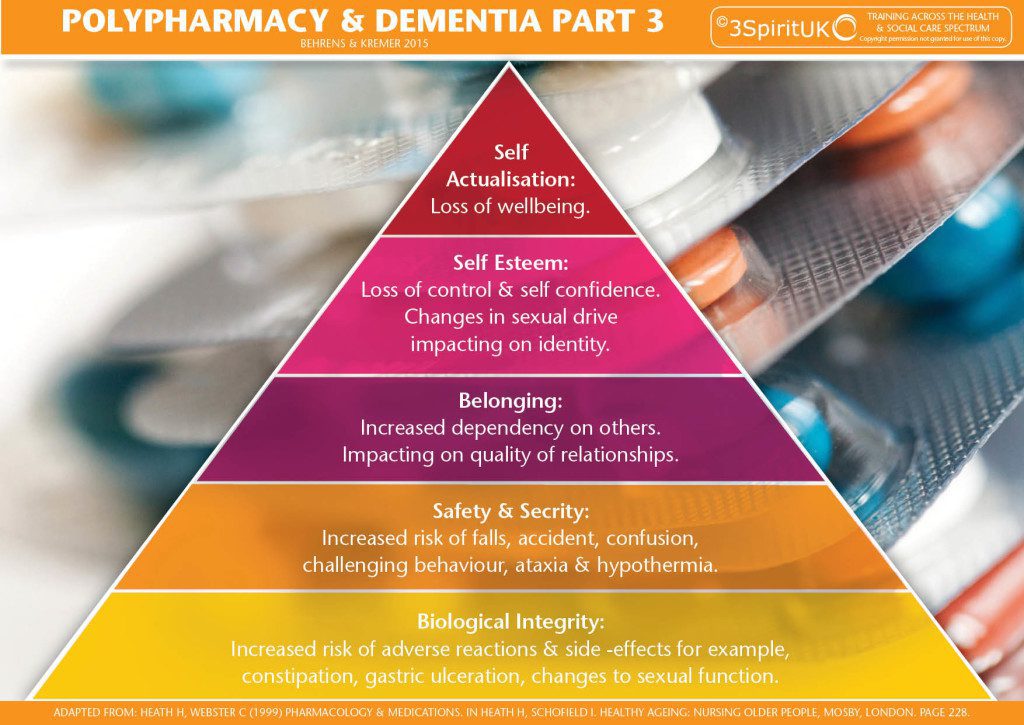
There are substantial risks of polypharmacy: for example, there may be severe side effects, some of which further compound cognitive challenges. There may also be drug-drug interactions and drug-disease interactions. The impact can be far reaching; Side effects may cause drowsiness leading to an increased risk of falls. There may be impacts on appetite and poor nutrition leading to multiple problems, not least a compromised immune system. Further than a physiological level, for example certain medications may impact on changes to sexual drive, impacting on identity and ultimately self-esteem. Changes in mood caused by the medication, coupled with cognitive difficulties may lead to emotional distress and challenging communication. In some instances the inappropriate use of medication can create the very problem that it is trying to solve.
There are many possible causes of inappropriate polypharmacy:
• Multiple physicians
• Self-medicating
• Over the counter medicines including herbal preparations
• Medicine dependent culture
• Medication administration errors
• Treating medication side effects with other medications: e.g. a medication may cause constipation, may then be prescribed a laxative. Alternatively maybe appropriate to consider non drug approach: diet.
When the side effects of medication are misdiagnosed as symptoms of another condition. Further medication is prescribed (Cascade prescribing), further side effects and unanticipated drug interactions may present. Older people with dementia who take a cholinesterase inhibitor and who experience urinary incontinence are more likely to receive an anticholinergic medicine to manage their symptoms
Drugs including some antidepressants, muscle relaxants, antispasmodics, and antihistamines may have anticholinergic effects and, therefore, may cause confusion, blurred vision, dry mouth, light-headedness, constipation, and difficulty with urination and/or loss of bladder control causing additional difficulties for a PWD.
Some examples from research:
In a prospective cohort study of 294 older people 22% percent of patients taking 5 or less medications were found to have impaired cognition as opposed to 33% of patients taking 6-9 medications and 54% in patients taking 10 or more medications.
Also in this paper: Polypharmacy affected patient’s nutritional status. A prospective cohort study found that 50% of those taking 10 or more medications were found to be malnourished or at risk of malnourishment
Jyrkka J, Enlund H, Lavikainen P, et al. Association of polypharmacy with nutritional status, functional ability and cognitive capacity over a three-year period in an elderly population. Pharmacoepidemiol Drug Saf. 2010;20:514–522. [PubMed]
A study in elderly patients with dementia reported that those patients who reported a fall had an increased prevalence of polypharmacy
Lee CY, Chen LK, Lo YK, et al. Urinary incontinence: an under-recognized risk factor for falls among elderly dementia patients. Neurourol Urodyn. 2011;30:1286–90. [PubMed]
American study
Two-thirds of hospitalisations for adverse events involved four medicines or classes — warfarin, insulins, oral antiplatelet agents or oral hypoglycaemic agents — taken alone or in combination
Budnitz DS, Lovegrove MC, Shehab N, et al. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 2011;365:2002–12. [PubMed]
References
All Party Parliamentary Group on Dementia (2008) Always a last resort: inquiry into the prescription of antipsychotic drugs to people with dementia living in care homes. Alzheimer’s Society. London.
Kleijer BC, van Marum RJ, Egberts AC, Jansen PA, Knol W, Heerdink ER. (2009). Risk of cerebrovascular events in elderly users of antipsychotics. J Psychopharmacol. Nov;23(8):909-14. Epub 2008 Jul 17.
NHS Information Centre (2012) National Dementia and Antipsychotic Prescribing Audit.
Gill SS, Mamdani M, Naglie G, et al. A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Archives of internal medicine 2005;165:808–13. [PubMed]
http://pathways.nice.org.uk/pathways/dementia
Deprivation of Liberty – Are we spending public monies wisely? Trish O’Hara April 2015
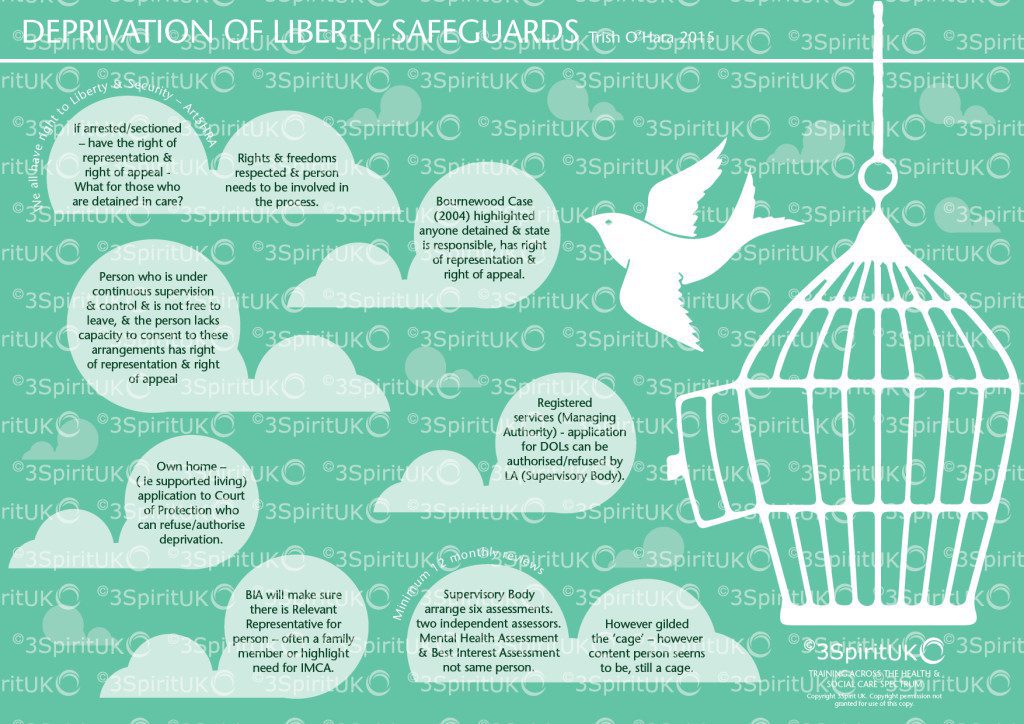
I for one, am fully aware of the necessity of adhering to Article 5 of the ECHR and delighted that Lady Hale pointed out that however golden the cage, it is still a cage.
But, the new threshold following the Cheshire West ruling :-
Continuous supervision and
Lacking capacity to consent to remaining
And how it falls within the Human Rights legislation:
The objective element: i.e. that the person is confined to a particular restricted place for a non-negligible period of time;
The subjective element, i.e. that the person does not consent (or cannot, because they do not have the capacity to do so) to that confinement;
State imputability: i.e. that the deprivation of liberty can be said to be one for which the State is responsible.
seems to have created an unprecedented amount of paperwork for those who, perhaps, need to be focused on emergency situations in hospital.
I am fully behind the new ruling for those living in residential care homes, nursing homes and hospices but am not sure this is money well spent on those in Intensive Care Units and in transportation from one hospital to another. It seems to me that those completing the assessments – such as Section 12 doctors and Best Interest Assessors are in the lucrative situation of charging £250 or so to assess people who are sick in hospital for a week or so. The nursing staff having to make applications, to spend time with the assessors – all of which is time away from using their expertise in keeping the person alive. I am aware that on many occasions, assessors have gone out to complete an assessment and the person has either gained capacity or indeed died or been discharged. I expect the assessors are still paid for their time and yet more public money is swallowed by this over-zealous interpretation of the ruling.
Of course, when a patient is resisting treatment and needing restraint, there needs to be protocols in place to ensure it is to maintain the life of the person, but can this not be regulated within ordinary hospital procedures?
Public monies are a dwindling resource as services face further cuts. Surely, there needs to be a common sense approach to deprivation and when it is necessary to authorise it.
I understand that new guidance is due to be published in 2017 which I hope recognises the paper driven exercise that often seems both pointless and expensive.
Yes, all patients should be informed and asked to sign consent for a time when they may not have capacity, following an operation and yes the MCA is a wonderful piece of law that protects the rights of all of us. But, the idea that a person who has suffered perhaps a head injury in a road accident and needs to take an ambulance for numerous hours to a specialist hospital needs a DOLs seems to me to be wasting peoples time and money.
I am not sure there is enough emphasis yet on getting this right where it needs more attention, time and money spent.
Are there enough home care providers who are involved in supporting a deprivation in a persons own home, not registered, trained in understanding liberty?
Do families understand that deprivation of liberty may be seen as false imprisonment?
Do enough care homes understand the right for people with capacity to make unwise decisions?
Do enough supported living services realise that they may need to apply to the court of protection if they are depriving a person of their liberty?
Surely, these are the areas of real concern. And where assessment and monitoring is most needed.
So the opening chapter of The Care Act is all about wellbeing. I presume every agency has wellbeing in their mission statement. We talk about wellbeing all the time in services today. It is the main driver of our delivery. It is how we are measured. It is the point. And yet, in my experience, practitioners struggle to define it.
Let’s be honest, care packages are created on the back of need, not want. Budgets mean that only ‘need’ is eligible. Any social worker who thinks their assessment processes are person centred must accept that their assessment processes are purely needs led. Person centred planning is aspirational and dreams led – it’s about want not need. What is important for the person is often in direct conflict to what is important to them. Whilst a person’s care package is based on need – the service providing said package is then measured on outcome. This means the provider must know how to move on from the initial assessment and turn the process on its head – still making sure that the person is in receipt of the service they are paying for.
This is not easy.
In essence, the budget meets the persons needs – but your service will be measured on the persons wellbeing and outcome.
So let us define outcome focused practice;
Input The resources required to provide agreed service
Activity The action plan that delivers said service
Output The service is evidenced as delivered
Outcome How this makes the person feel
An example to help us as follows;
Colin is a man with Down Syndrome and a mild to moderate learning disability. Colin has had a life long dream of meeting Elvis in Vegas. Colin lives with 5 others in a registered care home. Colin has the capacity to make his own decisions in the main and chooses to eat very surgery and fatty foods. Colin has diabetes and is about 5 stone overweight which is putting a great strain on his heart and effecting mobility. Colin often refuses his medication and has uncontrolled epilepsy with several seizures per day. Colin is very gregarious and friendly, often singing Elvis songs and making people around him feel good. The staff at his care service have spent years attempting to support Colin to make ‘better’ decisions about his diet and medication. He ignores them. Colins mum is very involved in his care and is worried about his health.
It is when Colin begins a person centred plan – using PATH that his life changes.
Starting with the dream – Colin is in Vegas meeting ‘an’ Elvis.
Colin has a hotel room and a ticket to an Elvis concert
Colin is on the plane with a ticket, passport and visa
Colin has saved £3500
Colin has permission from his GP and insurance to fly
We can see there are a myriad of barriers to this trip. We can see that there a many risks.
Colin tells the staff his dream – staff work from the dream to support Colin to take control over his life.
Colin is excited about going to Vegas. Colin takes his medication without fail and even agrees to a blood test. Colin actively involves himself in healthy eating and manages to lose 3 stone. Colin chooses to walk from the bus the final mile to the day service every day – this was his idea. Colin no longer drinks fizzy drinks. Colin is offered money from his mum and his uncle toward the trip. Colin saves and budgets toward his trip. Colin goes to see Elvis impersonators in the UK. The GP agrees that Colin is now fit to fly. Colin flies to Manchester to see family who he had lost touch with and to see how flying felt. Colin gets a passport.
Let’s use the language to describe events.
Input: Staff time – Actions plan creations – Appointments with health professionals
Action: Nutrition Plan, Exercise Plan, Budget/Savings Plan. Colin begins to shop, cook and eat according to plans – along with medical appointments, taking of his medication – controlling his epilepsy and blood sugars.
Output: Colin goes on his dream trip to meet an Elvis in Vegas
Outcome: Colin has outcome long before output – Colin takes control of his health, his diet, his life. Colin loses weight, becomes more active, controls his seizures and enjoysa full active life in his community. Colin makes plans, budgets and makes decisions.
It is often presumed that outcome comes after output, but as you can see by this example, often outcome arrives before output. In fact, Colin may never get to Vegas, (although I jolly well hope he does) – but still the outcome comes pouring in.
Staff have been working on Colins health and diet for years – but never before had Colin engaged in it. Colin needed to be heard. Colin wanted a trip to Vegas to meet Elvis, which was seen as impossible – Evidently, people believing in Colins dream and supporting him to work toward it – meant that he felt in control, empowered and made his own great steps to achieve his dream. The outcome is clearly filled with evidence of wellbeing.
It is this example that helps us think about what we measure. Output is not where we stop and is not what we measure. Wellbeing is outcome – and it is wellbeing that must be documented as evidence that we are providing the services that the person is paying for – Not need.